


CLINICAL BOTTOM LINE
Nasal saline irrigation may help relieve symptoms of allergic rhinitis (hay fever) in both adults and children when compared with no saline irrigation and is unlikely to be associated with adverse effects. It is unclear which is the best type of saline irrigation to use.
CLINICAL SCENARIO
Nasal irrigation – rinsing inside the nose – with saline water is commonly recommended for reducing symptoms of allergic rhinitis and can be used alone or as an adjunct to other therapies. As a ‘natural’ remedy it may be considered free of side effects. But is this procedure really a safe and effective way of relieving the symptoms of this troubling and common condition?
QUESTION
Does saline nasal irrigation reduce symptoms of allergic rhinitis in comparison with no saline irrigation?
SEARCH STRATEGY
PubMed – Clinical Queries (Therapy/Broad): saline AND allergic rhinitis
CITATION
Head, K., Snidvongs, K., Glew, S., Scadding, G., Schilder, A. G., Philpott, C., & Hopkins, C. (2018). Saline irrigation for allergic rhinitis. Cochrane Database Syst Rev, 6, Cd012597. doi:10.1002/14651858.CD012597.pub2
STUDY SUMMARY
A systematic review to evaluate the effects of nasal saline irrigation in people with allergic rhinitis. Inclusion criteria were:
Type of study: Randomised controlled trials (RCTs), cluster-randomised trials and quasi-randomised trials, and cross-over trials.
Participants: Adults and children with clinical symptoms characteristic of allergic rhinitis. Main exclusions were people with non-allergic or chronic rhinosinusitis; acute sinusitis; cystic fibrosis; immunotherapy within the prior year; aspirin-exacerbated respiratory disease.
Intervention: Saline, as an active treatment, delivered to the nose by any means (douche, irrigation, pulsed, spray or nebuliser) and with any volume, tonicity and alkalinity.
Comparison: (1) No nasal saline irrigation or (2) other pharmacological treatments
OUTCOMES
Primary outcomes: Disease severity, significant local adverse effects: epistaxis.
Secondary outcomes: Disease-specific health-related quality of life (HRQL), individual symptom scores, general HRQL, local irritation or discomfort, ear symptoms and nasal endoscopy scores.
STUDY VALIDITY
Search strategy: Comprehensive search strategy to locate published and unpublished studies. No language or date restriction.
Review process: Two authors independently screened the search results for eligible studies, selected the studies, extracted data using a standardised form, and conducted risk of bias assessment. Disagreements were resolved by consensus.
Assessment of risk of bias in included studies: Conducted using the Cochrane risk of bias tool.
Overall validity: A good quality review involving small studies of varying risk of bias.
STUDY RESULTS
Screening of 1,402 titles/abstracts and then 86 full text assessments identified 14 eligible RCTs. All studies reported outcomes under three months follow-up. Studies included children (seven studies, 499 participants) and adults (seven studies, 248 participants).
Saline volumes ranged from ‘very low’ to ‘high’ volume and used either hypertonic or isotonic saline solution, where reported. Only the results of the saline compared with no saline (our clinical question) are discussed here.
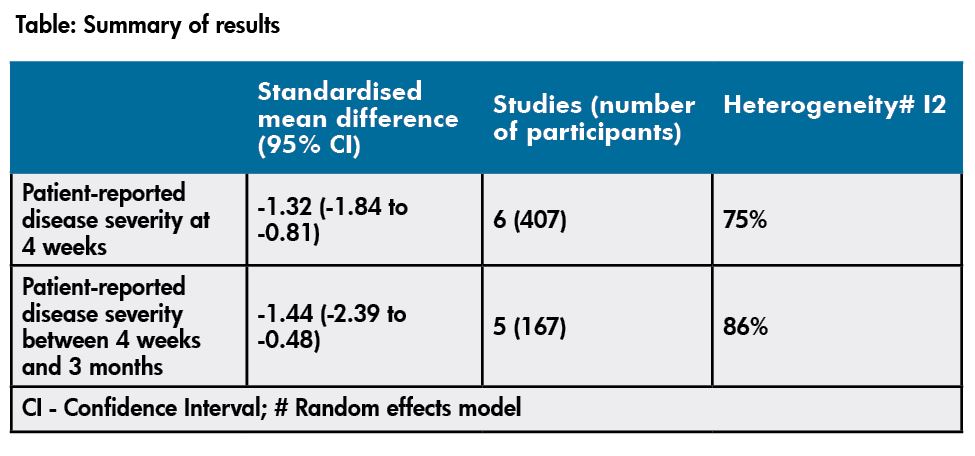
Studies used different scoring systems to report on patient-reported disease severity and so data was pooled using standardised mean difference (SMD). There was a statistically significant improvement in patient-reported disease severity in those who used saline irrigation compared with no saline at up to four weeks and between four weeks and three months (refer table).
Whether saline irrigation improves disease-specific HRQL is uncertain because just one small study reported this outcome.
Two studies (240 children) reported no adverse effects (epistaxis or local discomfort) in either group and only three reported no adverse effects in the saline group. No other prespecified outcomes were reported, other than those described here.
 COMMENTS
COMMENTS
- High heterogeneity between studies was appropriately investigated and partly driven by one small positive study. Evidence was low quality for all outcomes, which reflects uncertainty in the clinical bottom line.
- The standardised mean difference (SMD) at both four weeks and four weeks to three months were considered large effect sizes. The authors equated the SMD of -1.32 to a decrease of nearly two points on a ‘0 to 10’ point visual analogue scale (VAS) for nasal symptoms (lower = better). This seems clinically meaningful considering how miserable symptoms can make people feel. Improvement occurred in both adults and children.
- This review was not able to determine the best way of irrigating with saline, or the best strength of solution.
- Salty water is cheap and widely available and there are various options for getting it up your nose. Until we know more, it seems the best way is personal preference.
Reviewer: Cynthia Wensley PhD, RN, Lecturer, School of Nursing, University of Auckland
[email protected].


















